GM CASE 8
This is online E log book to discuss our patient's de-identified health data shared after taking his/her/guardian's signed informed consent. Here we discuss our individual patient's problems through series of inputs from available global online community of experts with an aim to solve those patients clinical problems with collective current best evidence based inputsThis e-log book also reflects my patient centered online learning portfolio and your valuable inputs on comment box is welcome".
A 60 year old Male who is a labour by occupation visited our opd which chief complaints of fever and cough since 15 days .
History of present illness:
Patient was apparently asymptomatic 3 years back then he developed fever associated with chills which is intermittent and also dry cough .He joined our hospital it got reduced and he discharged.before 15 days he again developed high grade fever associated with
Loose stools,low backache, burning micturation,sob.
No h/o abdominal pain, no h/o heamaturia.
So he visited local hospital but there is no use then he immediately joined our hospital.
Past history:
Patient suffered from similar complaints in the past.
No h/o diabetes
No h/o hypertension
No h/o epilepsy
No h/o TB
No h/o asthma
No history of any previous surgery in the past.
Personal history:
Appetite:decrease
Diet:mixed
Adequate:sleep
Bowel :loose stools
Bladder:normal
Occasionally alcohol and cigarette but stopped before 3years.
Family history:
No similar complaints in the family.
Drug history:
No allergy to known drugs.
General examination:
Patient is conscious,coherent, cooperative.
No pallor
No cyanosis
No lymphadenopathy
No clubbing
No icterus
No edema
No tremors
Temp: 101°f
Pulse rate:104/min
RR:29/min
Bp:110/80



Systemic examination:-
Cvs:
S1 and s2 are heard .
Respiratory system
No dysponea
Position of trachea central .
Abdomen:
No tenderness
No palpable mass
Bowel sounds are present.
CNS
Patient is conscious
Speech is normal
Provisional diagnosis:
Viral pyrexia,urinary tract infection.
Investigations:

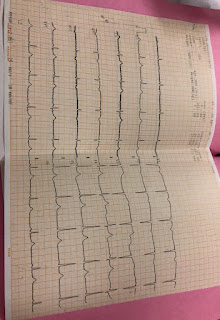





Treatment:
Inj pantop 40mg IV
Inj neomal 1gm iv
Tab dolo 650mg
Plenty of oral fluids
Syrup grllinctus 10mg po/bd



Comments
Post a Comment